John G. Taplin, Lea Bill, Ian E. Blanchard, Cheryl M. Barnabe, Brian R. Holroyd, Bonnie Healy and Patrick McLane
CMAJ Open: December 12, 2023 11 (6) E1135-E1147; DOI: https://doi.org/10.9778/cmajo.20230039
Abstract
Background: Prior work has shown that a greater proportion of First Nations patients than non–First Nations patients arrive by ambulance to emergency departments in Alberta. The objective of this study was to understand First Nations perspectives on transitions in care involving paramedics, and paramedic perspectives on serving First Nations communities.
Methods: Participants for this participatory qualitative study were selected by means of purposive sampling through author networks, established relationships and knowledge of the Alberta paramedicine system. First Nations research team members engaged First Nations community organizations to identify and invite First Nations participants. Four sharing circles were held virtually in July 2021 via Zoom by the Alberta First Nations Information Governance Centre. We analyzed the data from the sharing circles using a Western thematic approach. The data were reviewed by Indigenous researchers.
Results: Forty-four participants attended the 4 sharing circles (8–14 participants per circle), which ranged from 68 to 88 minutes long. We identified 3 major themes: racism, system barriers and solutions. First Nations participants described being stereotyped as misusing paramedic systems and substance using, which led to racial discrimination by paramedics and emergency department staff. Discrimination and lack of options to return home after care sometimes led First Nations patients to avoid paramedic care, and lack of alternative care options drove patients to access paramedic care. First Nations providers described facing racism from colleagues and completing additional work to act as cultural mentors to non–First Nations providers. Paramedics expressed moral distress when called on to handle issues outside their scope of practice and when they observed discrimination that interfered with patient care. Proposed solutions included First Nations self-determination in paramedic service design, cultural training and education for paramedics, and new paramedicine service models.
Interpretation: First Nations people face discrimination and systemic barriers when accessing paramedicine. Potential solutions include the integration of paramedics in expanded health care roles that incorporate First Nations perspectives and address local priorities, and First Nations should lead in the design of and priority setting for paramedic services in their communities.
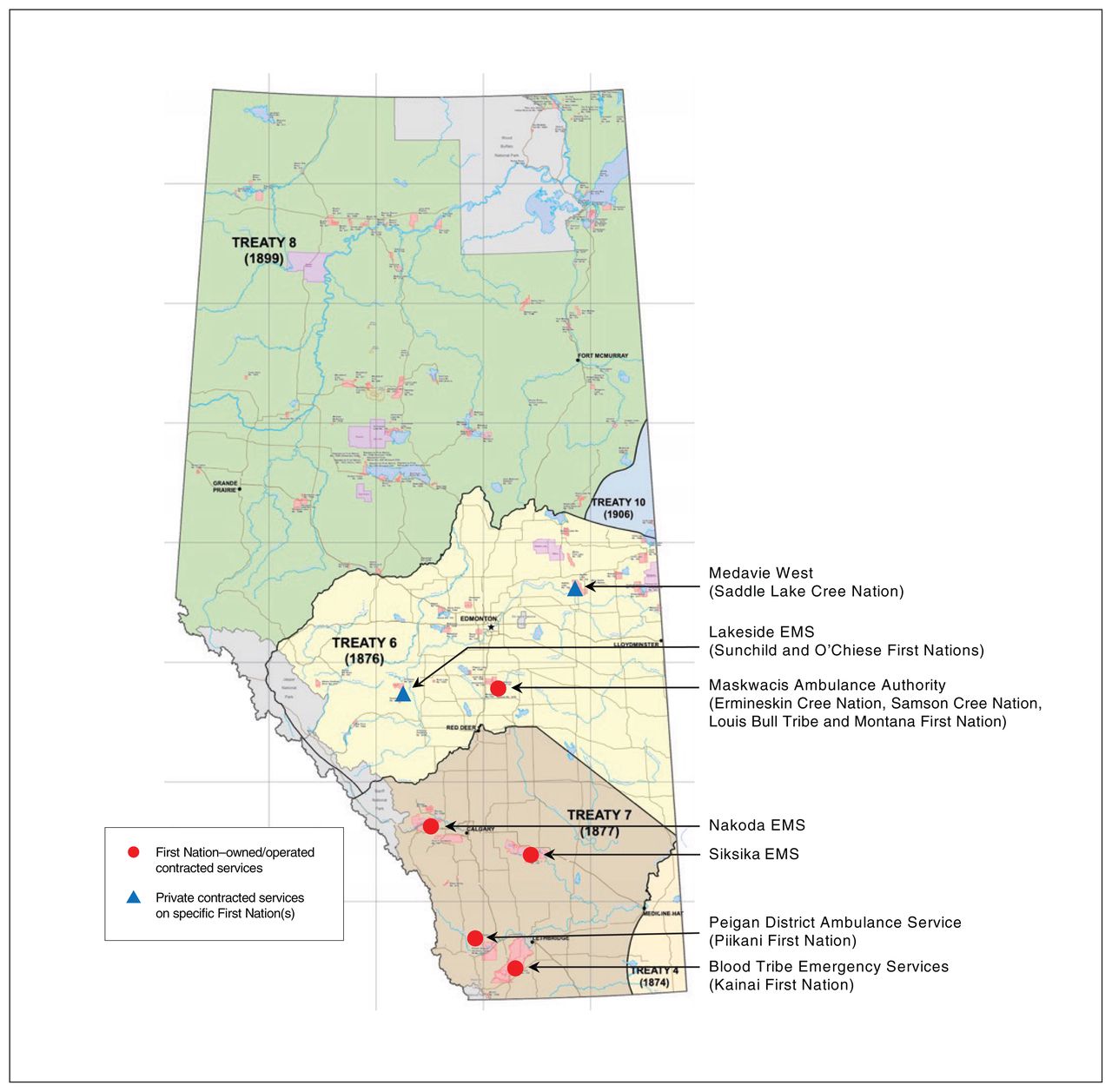
Alberta is subject to treaties that were negotiated between First Nations and the Crown as the legal basis for coexistence among Indigenous and settler peoples in Canada.1 The 3 main numbered treaty territories in Alberta are Treaty 6, in central Alberta, Treaty 7, in southern Alberta, and Treaty 8, in northern Alberta (Figure 1).2 Indigenous interpretations of treaties posit them as the basis for evolving peaceful and life-affirming coexistence. 3 Paramedicine is one field where settlers and First Nations are negotiating relations today. The definition of paramedicine is evolving,4 and paramedicine and paramedic services are undergoing extensive change.5 However, for the purposes of this paper, we use these terms interchangeably with terms such as emergency medical services (EMS) to refer to the system in which paramedics work.6 Paramedicine includes the conventional ambulance-based services provided by paramedics that involve responding to requests for emergency medical care, stabilization on the scene and transport to an emergency department (ED) for further care, as well as novel approaches to care that include integration of paramedics into the health care system.7 Community paramedics in Alberta are advanced care paramedics with additional training to manage nonemergent conditions in the community in consultation with medical providers.8 We use the term “providers” to refer to all health care providers and paramedics as a narrower term throughout this text.

{kind=link}
{kind=link}
Figure 1:
First Nations ambulance operators and treaty areas. Note: EMS = emergency medical services. Source: developed from the Government of Alberta First Nations reserves and Métis settlements map.2
A greater proportion of First Nations patients than non–First Nations patients arrive by ambulance to EDs in Alberta,9 and First Nations people face inequities when accessing acute care.10–12 In an institutional ethnographic work based in Calgary, Alberta, Corman13 quotes a paramedic who is intolerant toward “Natives,” and this racism is described as being learned on the job. The aim of the present study was to understand First Nations perspectives on transitions in care involving paramedics, and paramedic perspectives on serving First Nations communities.
Methods
Setting
The provincial health authority, Alberta Health Services (AHS), provides paramedic services in Alberta through direct delivery and contracted ambulance operators. There are 5 First Nations–operated ambulance services that provide services to specific First Nations (Figure 1). All other First Nations are serviced by AHS EMS direct delivery or private contracted services that respond from off-reserve.
Design
This was a participatory qualitative study guided by the concept of creating ethical space.14 As a team, we value both Western and Indigenous research approaches and understandings, using a community-based participatory research approach. In keeping with Indigenous methods presented by Kovach,15 we understand that our work is based in “a relational understanding of accountability to the world” and our communities. We co-constructed knowledge through interrelationships among our team members and an ethical engagement with participants. The Alberta First Nations Information Governance Centre (AFNIGC), a First Nations–led organization accountable to all First Nations in Alberta, was the lead organization for this study. The centre ensured adherence to the First Nations principles of Ownership, Control, Access and Possession (OCAP) of health data by securing qualitative and survey data on AFNIGC servers and performing all analyses in partnership with Western research team members.16
In October 2019, the research team met with Elders who had previously guided ED-related research. Consistent with previous studies, the Elders provided direction for the study conduct to ensure that researchers approached the study with respect and incorporated Indigenous values, knowledge and histories into the research design. We used the Consolidated Criteria for Reporting Qualitative Research checklist17 to guide the reporting.
Participant recruitment
We selected study participants using purposive sampling through author networks, as well as established relationships from previous research and professional knowledge of the Alberta paramedicine system. Through their established relationships, First Nations research team members engaged First Nations community organizations to identify and invite First Nations participants. We aimed to recruit First Nations community members with experience accessing paramedic care, paramedics with experience serving First Nations communities (within AHS, private services and First Nations paramedic services) and health care system leaders. We sought to ensure participation of people from different parts of Alberta, and those of varying ages and genders.
Data collection
Four sharing circles were held virtually in July 2021 via Zoom videoconferencing software (version 5.7.1), which is a validated method for qualitative data collection.18 Sharing circles are an Indigenous method whereby issues of common interest are discussed and all participants are viewed as equal in a supportive and healing environment that is respectful to Indigenous protocols.19 Virtual sharing circles have been previously reported in a qualitative study of the experiences of Indigenous nursing students during the COVID-19 pandemic in which the author adopted Indigenous and Western methods.20 Before the sessions, participants completed online consent forms or provided verbal consent by telephone, and completed a demographics questionnaire. In the questionnaire, participants indicated whether they were attending as community members or as people involved in paramedic services. The data collection sessions began with Elders offering a prayer, followed by a discussion of voluntary participation and participant withdrawal procedures, as well as a description of the project objectives. L.B. and P.M. facilitated the sharing circles. They were positioned to facilitate dialogue using elements aligned with an Indigenous conversational methodology that was based on the tradition of knowledge sharing and oriented to Indigenous ways of knowing.15
To encourage dialogue and to prompt participant discussion in an unstructured and open way, L.B. created a graphic showing the transitions in care that patients experience during paramedic care that was presented to sharing circle participants (Figure 2). The experience is depicted as a circle because our team’s prior experience is that patients often have multiple transports and encounters with EMS over the course of a health event.

{kind=link}
{kind=link}
Figure 2:
Transitions in care that patients experience during paramedic care. Note: EMS = emergency medical services.
Analysis
Recordings were transcribed verbatim, and AFNIGC staff verified the accuracy of anonymized transcripts. The data were de-identified by AFNIGC and held securely on AFNIGC servers. The anonymized data were shared with investigators for analysis. The primary analytic team included a settler paramedic researcher (J.G.T.), a settler paramedic research leader (I.E.B.), a First Nations researcher and knowledge holder (L.B.) and a settler sociologist with qualitative methods expertise (P.M.). Transcripts were coded thematically. 21 Coauthors contributing to the study design, data interpretation and critical revision of the manuscript included a First Nations registered nurse/trauma-trained ED nurse (B.H.), a settler emergency physician with senior leadership roles (B.R.H.) and a Métis specialist physician with expertise in Indigenous health research (C.M.B.).
J.G.T. coded transcripts in NVivo 11 (QSR International), informed by guidance from L.B. and a previous ED study led by P.M. and L.B.10 Themes were developed in consultation with the research team and were revised during manuscript drafting. Results of the analysis were presented to 2 First Nation Elders and a health care technician identified by the research team in October 2022, and their feedback is reflected in the data interpretation. The Elders’ perspectives guided us to consider the results in relation to First Nations values that did not originally form part of our interpretations.
Ethics approval
The study received ethics approval from the Health Research Ethics Board of Alberta Community Health Committee (HREBA.CHC-19–0074) and the University of Alberta Health Research Ethics Board (Pro00098744).
Results
Forty-four participants attended the 4 sharing circles (8–14 participants per circle), which ranged from 68 to 88 minutes long. The attendees included First Nations community members, paramedics and EMS managers from all treaty areas (Table 1) (additional demographics questionnaire responses are provided in Appendix 1, Supplementary Tables S1 and S2, available at www.cmajopen.ca/content/11/6/E1135/suppl/DC1). Experiences were predominantly from paramedics and others providing health care services on First Nations reserves (Appendix 1, Supplementary Tables S2 and S3). Three themes were identified: racism, system barriers and solutions. In addition, 20 subthemes (8 subthemes of racism, 6 subthemes of system barriers and 6 subthemes of solutions) were identified (Figure 3).
Table 1:
Participant characteristics

{kind=link}
{kind=link}
Figure 3:
Themes and subthemes identified. Note: ED = emergency department, EMS = emergency medical services.
Racism
Participants described racism in terms of ideas about and actions toward First Nations members that limited their access to quality paramedic care (Table 2). In particular, racist stereotypes related to perceived misuse of EMS and substance use, race-based discriminatory treatment by paramedics and at EDs, and racism toward First Nations health care providers. Descriptions of stereotypes of ED misuse were complicated by participants’ efforts to delineate what constitutes true misuse of EMS.
Table 2:
Racism subthemes, with illustrative quotations
System barriers
In each sharing circle, community members, paramedics and health care system leaders identified a lack of primary care on-reserve as a major contributor to EMS use (Table 3). Health care system leaders included First Nations health care directors, and senior health care providers, administrators and managers from various disciplines that interface with paramedic services. Many participants described that lack of resources for after-hours care necessitates EMS and ED use for nonemergent medical conditions. Participants also described system issues that arise from a lack of coordination between First Nations and non–First Nations health care and transportation systems, including paramedics’ difficulty navigating First Nations reserves, paramedic services bills’ being sent to collection agencies (even when the patient is insured) and lack of effective mechanisms to report discrimination. Some participants also described the way system-driven response times negatively affect care interactions. Among the most striking results were descriptions of patient avoidance of care and attempts by paramedics to advocate for patients within the wider health care system.
Table 3:
System barriers subthemes, with illustrative quotations
First Nations community members and paramedics identified that First Nations patients may be reluctant to be transported for care. Avoidance of care was predominantly expressed as being related to negative past experiences in EDs and system barriers that create difficulties returning home. Respondents indicated that, when deciding to seek care, First Nations people weigh the severity of their illness against their ability to access transport home after transport to and care in an ED.
Paramedics expressed distress associated with their inability to perform duties when patient avoidance of care is founded on previous experiences of discrimination. A paramedic leader described a case in which a patient died after refusing transport to hospital based on previous discrimination there. Paramedics also spoke about frustration with the lack of consistent care delivered in EDs and negative attitudes toward First Nations peoples. One paramedic (P27) described that it is emotionally difficult to be “the gateway between the bad experience you’re currently having and another bad experience that you’re going to have from people that are expected to help you.” Some paramedics described themselves as advocates for patients within the wider health care system, in some cases citing their greater familiarity with particular patients.
Solutions
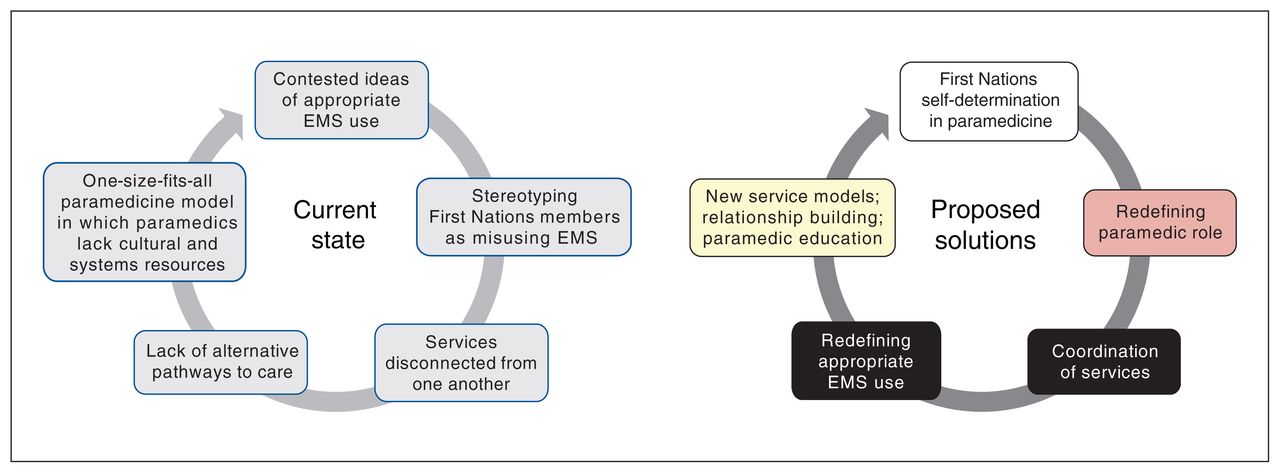
Participants described potential solutions to issues in paramedic care for First Nations people, including practitioner cultural training and education; building relationships and partnerships with First Nations communities and the organizations that serve them; developing new service models; First Nations self-determination in paramedic service design; and coordination of services (Table 4, Figure 4).
Table 4:
Solutions subthemes, with illustrative quotations

{kind=link}
{kind=link}
Figure 4:
Current state of and proposed solutions to barriers First Nations people encounter when accessing emergency medical services (EMS) in Alberta.
First Nations community members and EMS operators expressed the importance of First Nations self-determination in health care services, including EMS. Participants from First Nations communities stated that their priorities for EMS may be distinct from those of the provincial health authority.
One participant powerfully described that appropriate use of EMS is a contested matter:
I think the definition of proper use of an ambulance is constructed within White communities that have access to hospitals quite readily. We need to work on redefining what the appropriate or proper use of ambulance services is in remote Indigenous communities [and] even in not so remote Indigenous communities. There needs to be a change in paradigm or just a redefinition of what exactly that means. — P22, EMS manager
When asked for solutions to the challenges of EMS on First Nations, some participants suggested patient navigation, wraparound services in collaboration with other health care services, and inclusion of Indigenous knowledge holders in design and delivery of health care services as key priorities. Participants also discussed the opportunity for community paramedic programs to address nonemergent conditions as part of a multidisciplinary care team. Community members recommended solutions for transport home from hospital that included after-hours transport.
In our meeting to discuss the results of the analysis with Elders, they reflected that the project was valuable and that they believed our results would drive positive change. They expressed a desire for community members to know that work is ongoing to improve paramedicine for First Nations in Alberta. They also emphasized the importance of First Nations values and principles (such as the Cree guiding principle for health of Kisêwâtisowin [“absolute compassion”]22) for local paramedicine services and the fact that First Nations members have a treaty right to health, as expressed in Treaty 6.23 Finally, the Elders noted that those in the health care system should think of future generations and recognize that, when they do harm, future generations will have to pay the price.
Interpretation
Our findings suggest that paramedic judgments of and behaviour toward First Nations community members in Alberta result in patient avoidance of care and contribute to negative health outcomes. In turn, paramedics themselves are negatively affected by witnessing the discrimination that First Nations patients encounter. Definitions of appropriate and inappropriate EMS use are at the core of conflicts observed in our study.
We found that stereotypes about First Nation members; experiences of discrimination by First Nations patients and paramedics and other care providers; patient avoidance of care; and system barriers to care all affect paramedicine in Alberta. We also found that paramedics are distressed when they are unable to provide care or ensure quality care by other health care professionals, and view themselves as patient advocates. Participants described potential ways to improve care of First Nations members, including First Nations–run health care services, coordination among services, support for culturally safe care through education, and new service models such as alternative care destinations, telehealth and community paramedics.
There are profound occurrences of discrimination and racism when First Nations people access ED care in Alberta.9–11 Our findings show that many issues that First Nations members encounter in EDs, including discrimination related to stereotypes about “misuse” of health care services and about substance use, also affect paramedic care.9–11
Authors of previous sociological studies of emergency medicine have argued that ED care is not simply medical but also involves moral judgments of patients.12,24,25 Our results show that this dynamic extends to paramedicine. Paramedics in our study were deeply invested in defining their role and describing which types of patients they should be seeing, although there was disagreement on definitions.
Corman26 performed an institutional ethnographic work similar to our study and reported that paramedics in Calgary classified ambulance events as “shit” when these were not viewed as legitimate or “true” emergencies. He argued that paramedics construct what they define as a “good” or “bad” call based on a variety of factors, including social categories. Likewise, in his ethnographic work in urban California, Seim27 reported that paramedics prefer “legit” over “bullshit” cases. “Legit” cases are defined by a need for relatively urgent medical intervention (e.g., related to serious vehicular trauma or diabetic episodes), whereas “bullshit” calls are related to social ills (e.g., lack of access to primary care, need for shelter). The latter require little medical care and potentially lead to unnecessary transport. As in our study, in which paramedics often understood that patients called for EMS because no other options were available, Seim27described paramedics as sometimes sympathizing with patients while defining many ambulance calls as “bullshit.” He argued that paramedicine is more than a job for many who do it; instead, it is a vocation or calling involving socially valuable work through which paramedics often define their core self-identities. We observed similar investment in paramedicine in our study when paramedics describe their role in advocacy for patients and the distress they experience when they are unable to provide or ensure needed care.
The problems identified in this study are predominantly systemic and thus require expansive, principle-based solutions. As each First Nation is sovereign and unique, we propose deliberately broad solutions amenable to adaptation to address local contexts and First Nations’ priorities. Further research could entail engaging policy-makers to identify and evaluate specific actions and resource allocation that promotes self-determination and addresses inequities, such as the development and implementation of community-led initiatives and advancing culturally safe practices. Furthermore, to ensure that all patients are safe when accessing paramedic services, organizations must focus on redefining appropriate emergency care use to be responsive to patient needs in the context of health care systems that do not serve all patients equitably. As one of our participants noted, the definition of appropriate access to EMS has been “constructed within White communities” and for patients with ready access to comprehensive health care services. Redefining how paramedics view their role could improve care interactions and promote referrals to necessary services, including primary care.
Alongside redefining definitions of their role, paramedic services must combat racism toward First Nations people by implementing cultural safety training28 that attends to the way care systems have been defined to privilege White communities and patients. This training should be led and evaluated in partnership with First Nations patients and community members.
However, respecting First Nations teachings through action and change in behaviours is the responsibility of settlers, who must focus on recognizing the value that First Nations ways and providers bring to their organizations. For instance, our results suggest that First Nations paramedics face the additional burden of acting as informal cultural mentors to non–First Nations providers, and this should be recognized and compensated.
Moreover, care locations to which paramedics transition patients (primarily EDs) must become culturally safe for First Nations patients in order for paramedics to fulfill their duty of care. At the same time, secure, sustained and equitable funding for First Nations primary care and other services will be essential in reducing mismatches between patient need and paramedics’ professional sense of themselves. A more robust care system can support the changes to paramedic definitions of their professional role and greater integration of paramedicine with the health care system, if supported by investment in paramedic training, community partnerships and program development.
The changes we recommend reflect the evolving practice of many paramedic services that incorporate paramedic care as part of an interdisciplinary team.5,29–31 Perhaps more important, recognizing First Nations self-determination in paramedicine aligns with the United Nations Declaration on the Rights of Indigenous Peoples.32 First Nations service providers can be key leaders in health care system transformation if they are supported and compensated to do this work, and if the paramedic profession is made safe for them. It is reasonable to regard the solutions we recommend as the basis of a model for serving First Nations communities.
Limitations
First Nations participants who do not have experience working in the health care system are underrepresented in our study. First Nations people without health care backgrounds may have perspectives and experiences different from those presented in this study. Youth are also underrepresented in our sample, with the majority of participants being older than 40 years.
Conclusion
First Nations peoples face discrimination and systemic barriers when accessing paramedic care. The integration of paramedics in expanded health care roles that incorporate First Nations perspectives and address local priorities and principles has the potential to alleviate many of the negative experiences that First Nations members face when accessing health care services. First Nations should lead in the design of and priority setting for paramedic services in their communities.
Footnotes
- Competing interests: The Alberta First Nations Information Governance Centre received a grant from the Canadian Institutes of Health Research (grant 414394) to support the conduct of this study. John Taplin, Ian Blanchard and Patrick McLane are employed by Alberta Health Services (AHS), a provider of emergency medical services in Alberta. Brian Holroyd is contracted to serve as the senior medical director of the AHS Emergency Strategic Clinical Network. John Taplin was paid as a research assistant for drafting the manuscript. He has received consulting fees from Siksika Health Services related to the development and implementation of a community paramedic program on a First Nation in Southern Alberta. No other competing interests were declared.
- This article has been peer reviewed.
- Contributors: Patrick McLane, Ian Blanchard, Lea Bill, Brian Holroyd, Cheryl Barnabe and Bonnie Healy conceived and designed the study. Patrick McLane provided qualitative methods direction, contributed sociological theory and led revisions to the theme structure. Patrick McLane, Lea Bill, Ian Blanchard and John Taplin acquired the qualitative data. John Taplin analyzed the data and drafted the manuscript. All authors contributed to data interpretation, revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
- Funding: The study was funded by a grant from the Canadian Institutes of Health Research (grant 414394).
- Data sharing: Access to original data may be requested through the Alberta First Nations Information Governance Centre.
- Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/6/E1135/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- ↵
- Starblanket G
- ↵(2021) First Nations reserves and Metis settlements (Government of Alberta, Edmonton) Available: https://www.alberta.ca/map-of-first-nations-reserves-and-metis-settlements. accessed 2022 Mar. 2.Google Scholar
- ↵
- Starblanket G
- ↵
- Williams B,
- Beovich B,
- Olaussen A
- ↵
- Tavares W,
- Allana A,
- Beaune L,
- et al.
- ↵(2006) The future of EMS in Canada: defining the new road ahead (Emergency Medical Services Chiefs of Canada, Calgary), p 3.Google Scholar
- ↵
- Drennan IR,
- Blanchard IE,
- Buick JE
- ↵
- Blanchard IE,
- Kozicky R,
- Dalgarno D,
- et al.
- ↵
- McLane P,
- Barnabe C,
- Holroyd BR,
- et al.
- ↵
- McLane P,
- Bill L,
- Barnabe C
- ↵
- McLane P,
- Barnabe C,
- Mackey L,
- et al.
- ↵
- McLane P,
- Mackey L,
- Holroyd BR,
- et al.
- ↵
- Corman MK
- ↵
- Ermine W
- ↵
- Kovach M
- ↵(2022) Ownership, Control, Access, and Possession (Alberta First Nations Information Governance Centre, Edmonton).Google Scholar
- ↵
- Tong A,
- Sainsbury P,
- Craig J
- ↵
- Archibald MM,
- Ambagtsheer RC,
- Casey MG,
- et al.
- ↵
- Lavallée LF
- ↵
- Van Bewer V
- ↵
- Vaismoradi M,
- Turunen H,
- Bondas T
- ↵
- Littlechild D
- ↵(1964) Copy of Treaty no 6 between Her Majesty the Queen and the Plain and Wood Cree Indians and other Tribes of Indians at Fort Carlton, Fort Pitt and Battle River with adhesions (Queen’s Printer, Ottawa) Cat. no. R33-0664. Available: https://www.rcaanc-cirnac.gc.ca/eng/1100100028710/1581292569426#chp1. accessed 2022 Oct. 28.Google Scholar
- ↵
- Hillman A
- ↵
- Vassy C
- ↵
- Corman MK
- ↵
- Seim JD
- ↵
- Ramsden IM
- ↵
- Whalen S,
- Goldstein J,
- Urquhart R,
- et al.
- Allana A,
- Kuluski K,
- Tavares W,
- et al.
- ↵
- Chan J,
- Griffith LE,
- Costa AP,
- et al.
- ↵(2007) Declaration on the Rights of Indigenous Peoples (United Nations, New York).Google Scholar
- © 2023 CMA Impact Inc. or its licensors